Obsessive-compulsive disorder (OCD) is a debilitating mental health condition that’s believed to affect at least 500,000 Australians, with adolescents representing a significant portion of those affected. Generally misunderstood in the community, people who have OCD don’t simply have a penchant for tidiness – they have a variety of unwanted obsessions that can cause significant stress and anxiety unless there is some intervention.
OCD? Not Me! is a free, online treatment program developed by Curtin University researchers that seeks to help young people aged 12–18 years with OCD.
Based on Exposure and Response Prevention – the gold-standard treatment for OCD – the program challenges participants to climb the metaphoric ‘OCD Mountain’ and gradually reduce the use of compulsive rituals to reduce their anxiety.
“People with OCD experience obsessions that are hard to dismiss and cause significant anxiety and distress. These include thoughts they are contaminated with germs, vivid images of something terrible happening to a loved one or thoughts they are a bad person. It is important to note these thoughts are unwanted,” explains lead researcher Professor Clare Rees.
“In response, the individual usually completes repetitive behaviours – compulsions – to reduce their distress. For example, if the intrusive thought is their mum getting sick, the young person might complete mental rituals, such as repetitively thinking ‘I love you, mum’.
“Schoolwork can also be affected; a young person might be caught up in writing perfect sentences because they have the fear that if they don’t something terrible may happen to a loved one.
“Unfortunately, what happens is that the person then falsely believes they must do a checking ritual to prevent the feared outcome.”
The OCD? Not Me! program tackles these compulsive rituals in eight stages, based on Exposure and Response Prevention treatment modules, from ‘Getting Ready’ to ‘Base Camp’ and all the way to ‘Reaching the Summit’.
As each stage is completed, parents are simultaneously given supplementary resources to ensure they understand their child’s symptoms.
The Curtin-led program is unique because it is fully automated, meaning participants do not have to interact with a therapist. Rees says this automation, along with the program’s interactive elements, have been key to its success.
“There are a number of significant obstacles to accessing evidence-based treatment for OCD. These include a lack of clinicians with expertise in treating the disorder, long waiting lists, cost of treatment and, in many cases, the practical difficulty and the fear participants have of attending face-to-face sessions,” Rees explains.
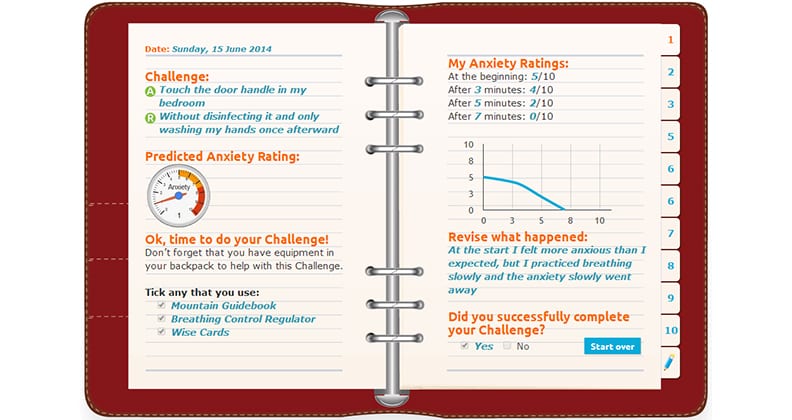
“We are aiming to make effective treatment more easily available to greater numbers of young people, before the problem becomes more entrenched and difficult to shift. Exposure with Response Prevention means we start by asking somebody with OCD to wash their hands for eight minutes, instead of 10 minutes, and so on.
“We want young people to see OCD as a challenge they can overcome as opposed to a medical condition they are stuck with, so that’s why we structured the program to feel like an adventure.
“We also renamed some common therapeutic strategies to fit in with the metaphor of a mountain climbing expedition; for example, controlled breathing became the ‘Breathing Control Regulator’ and psychoeducation became ‘Mountain Guidebook’.”
The research project began in 2013 after Rees and her team – fellow Curtin researchers Dr Rebecca Anderson and Dr Amy Finlay-Jones – were awarded more than $460,000 from the Commonwealth Department of Health. This number later increased to $640,000 as the department chose to extend the funding.
The team decided on an open trial design, as opposed to a controlled trial design, to directly compare the symptoms experienced by the young people from before they participated in the program to when they finished it.
Overall, more than 50 young people completed the majority of the program, with the research team observing that the participants’ OCD symptoms decreased in intensity over the duration of the program.
“We found the program resulted in statistically and clinically significant reductions in the severity of symptoms, as well as reductions in the amount of interference the symptoms cause in daily life, such as getting to school on time or the amount of time needed to take a shower,” Rees says.
Rees’ team are now planning the next phase of the research, where they are hoping to create two apps based on the OCD? Not Me! program: one for clinicians working with young people and one for the young people themselves.